
When one of the herpes viruses, herpes simplex 1 or herpes zoster, manifests in the eyes, it is called ocular herpes or herpetic eye disease. Ocular herpes may cause scarring, chronic inflammation, lesions, and ulcers that damage different layers of the cornea. It is the most common infectious cause of corneal blindness in the U.S.
Many people become infected with one of these viruses during childhood; they can be passed from one person to the other because the virus is contained in the moist skin that lines the mouth. In many people, the primary infection does not cause any symptoms. The most common time for a first active infection is between the ages of 30 and 40, and it may be more common in people who wear contacts. Because it affects the nerves directly, herpetic eye disease can be very painful.
Both viruses never leave the body after an initial infection; this can result in periodic flare-ups through one’s life, causing potential pain, including in the face and eyes. It is not known why the virus can suddenly flare-up, but it may be due to stress, low immunity, and/or trauma.
Most flare-ups will resolve within a few weeks in non-immunocompromised people, and in some, flare-ups can recur through one’s lifetime, possibly posing sight threatening eye problems.
What is Ocular Herpes?
Herpes simplex keratitis occurs when the herpes simplex 1 virus (HSV) infects the cornea or the white part of the eye. The term keratitis means an inflammation of the cornea. The virus first attacks the corneal epithelium, the thin outer layer of the cornea. This layer plays an important role in protecting the eye. It blocks intrusion from foreign materials and provides a smooth surface to absorb oxygen and cellular nutrients that are delivered through the tear film that lies on top of it. The epithelium also contains many nerve endings; it’s very sensitive.
When a virus attacks the cornea, this outer epithelium layer becomes red, irritated, and painful, because the nerve endings serving the cornea also become infected. The extent of damage can vary widely, sometimes healing by itself within a week to ten days. If the virus recurs at a latter time, however, the results can be more serious, including ulcers and lesions that extend to the stroma layer of the cornea. The stroma layer is a thick layer comprised of water, layers of protein fibers, and cells delivering nourishment.
There are two major types of this virus. Type I is the most common and is not sexually transmitted, while Type II typically infects the genitals. Of the two types, Type I more commonly affects the eye, often resulting in symptoms such as eye infections, cold sores, or blisters.
Herpes zoster ophthalmicus, which has initial symptoms that may be similar to herpes simplex keratitis, occurs when the varicella zoster virus, dormant in most people, attacks the ophthalmic nerve. It spreads to the epithelial layer of the cornea, then to the stroma layer. In 40–50% of cases, anterior uveitis also develops. Skin rashes around the eyes are another characteristic result.
Types of Occlusion
Two types of viruses are found: herpes simplex 1 (cold sores, herpes) and varicella zoster (chicken pox, shingles), causing herpes simplex keratitis and herpes zoster ophthalmicus, respectively.
Herpes simplex 1 virus is common; 50–80% of Americans carry the antibodies, depending on the socioeconomic group, and ocular infection from this virus affects about .008% to .03% of the population.
Varicella zoster virus was once very common; in the pre-inoculation era, 95% of children had the varicella antibodies before age 20. It is still carried by about 20% of the population. About 1% of these people develop herpes zoster ophthalmicus.
Types of Ocular Herpes
Herpes Simplex Keratitis (HSV)
Primary HSV. Once a person is infected, this virus may manifest as herpes simplex 1 or become dormant. If dormant, it remains dormant until some stress triggers an outbreak. This initial outbreak is rarely noticed and rarely affects the cornea. Sometimes a patient will have an episode of conjunctivitis or blepharitis that resolves itself.
Recurrent HSV. If HSV recurs, it most often affects the cornea, resulting in herpes simplex keratitis. Although it usually affects the cornea, it can cause retinitis, trabeculitis (inflammation of the trabecular meshwork), anterior uveitis, and optic neuritis.
Epithelial keratitis. This is the most common and mildest form. It affects only the top epithelial layer of the cornea. Inflammation of the epithelial layer of the cornea takes the form of several types of sores or ulcers. They are identified according to their shape and location.
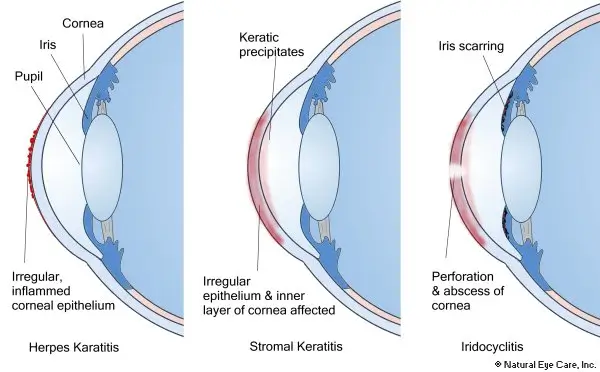
Stromal keratitis. Inflammation of a deeper layer of the cornea, the stroma, is more often associated with immune system issues; it can be quite serious, resulting in permanently blurred vision and blindness. It can manifest as a wide range of interrelated conditions. Some of these include interstitial keratitis (affecting spaces between cells), necrotizing keratitis, disciform keratitis (disc-shaped corneal swellings), and keratouveitis (uveitis predominates). Stromal keratitis develops in about 25% of those people who have epithelial keratitis.
Recurrence. Recurrence of epithelial or stromal keratitis is 10% after 1 year, 23% after 2 years, and 50% after 10 years.
Herpes Zoster Ophthalmicus (HZ)
Unlike the HSV virus there has been very little published research into natural complementary care for HZ. Because of vaccine use, it has become more rare. Like the herpes simplex 1 virus, the herpes zoster virus can cause an initial outbreak, or it can remain dormant in the body. If there is a recurrence, often triggered by emotional or environmental stress, not only the skin (shingles) but the cornea can be impacted. And, like the herpes keratitis, the epithelial or stroma layer can be affected.
Epithelial punctate. Epithelial erosions manifest with ulcers or lesions on the surface of the cornea.
Nummular keratitis. If the stroma layer is involved, it is called nummular keratitis, which occurs with granular deposits in the stroma layer, or necrotising interstitial keratitis, which occurs with leaking into the stroma, corneal thinning, and sometimes perforated cornea.
Disciform keratitis. This form displays corneal edema, and it folds in the Descemet’s membrane.
Neurotropic. This form involves damage to the nerves in the cornea, causing corneal damage, thinning, and sometimes perforation.
Iridocyclitis or anterior uveitis. These can develop from the zoster virus. Not only is the cornea affected, but also the deeper tissues of the iris is affected that causes severe light sensitivity, blurred vision, pain, and redness.
Symptoms
Ocular herpes is characterized by a painful sore on the eyelid or on the surface of the cornea of the eye.
- Infection of conjunctiva and eyelids that heals without scarring
- Recurring eye infections
- Irritation
- Pain
- Blurry vision
- Swelling
- Redness and sores
- Tearing and discharges
- Eye sensitivity and light sensitivity
There are a few other symptoms that help differentiate between the two forms. Herpes Simplex Keratitis
- A feeling of grit or dirt in the eye
- Tearing and discharge
- Pain, especially when looking at bright light
- Conjunctiva infection that heals without scarring
Herpes Zoster Ophthalmicus
- Headache and fever
- Rash or sores on forehead, eyelids, around the eyes, and sometimes the tip of the nose
- Blurry vision
Conventional Treatment (HSV)
Treatment depends on the form of the condition. Initial treatment is with either topical eyedrops or oral antiviral medication which is the cornerstone of topical treatment for herpes simplex keratitis. Treatments typically last 1–2 weeks, depending on healing time. However, resistence to antiviral medications (such as Acyclovir1) is an increasing problem. In mouse models there is promised of a vaccine for herpes simplex virus.2
Eyedrops called corticosteroids can help control the disease, but they can also raise the pressure in the eyes for some people, in which case additional eyedrops may be prescribed along with the corticosteroids to keep the pupil dilated that helps prevent the eye pressure from increasing due to corticosteroids.
In certain less-common cases, intravenous medication may be necessary, using antiviral drugs such as Acyclovir, and more recently Valacyclovir, to suppress the reproduction of the virus. Multiple treatments with steroids may be required if the middle layer of the cornea (herpetic stromal keratitis), back layer of the cornea (herpetic endotheliitis), and/or the iris (herpetic iritis) are affected.
Herpetic iritis is also treated with aggressive steroid use, including hourly prednisolone acetate and cycloplegia as cornerstone therapies.