 info@naturaleyecare.com
info@naturaleyecare.com



 Home
Home


 Vision
Vision Vision
Vision



 Health
Health Health
Health Research/Services
Research/Services Pets
Pets About/Contact
About/Contact
Lattice Degeneration
Vitamins/Supplements What it is Where it occurs Progression Symptoms & Causes Treatment Self help Reviews
Lattice degeneration gets its name from the crisscrossing, fine, white lines on the surface of the retina, which an eye doctor can see during examination. It occurs in 7–8% of the general population, most often in patients with myopia (nearsightedness) and over the age of 20. It also appears that neither race nor sex is a risk factor. Approximately 45% of those affected have lattice degeneration in both eyes. Patients with lattice degeneration are typically symptom-free.
What is Lattice Degeneration?
Lattice degeneration occurs when the outside edge of the retina (away from the central macula), responsible for peripheral vision, shrinks, thins, develops holes, or otherwise atrophies. Clinical features may include retinal thinning, branching, whitish lines on the retinal surface, and even small holes in the retina. In addition, lesions can form.
Sometimes lesions cause holes or breaks in the retina, which are atrophic in nature. Atrophic means that they are due to the wasting away or diminishing of portions of the retina. Unlike retinal detachment, these breaks and holes are not associated with pulling between the vitreous and retina. They are usually an incidental finding of a dilated ophthalmologic examination that may occur within the lattice (present in 25–35%) and result from progressive retinal thinning. The fine lines seen in lattice degeneration are present in roughly only 10% of all lesions. The other 90% are known as uncomplicated lattice degeneration, with lesions but no tears, holes, or breaks.
Where Does it Occur?
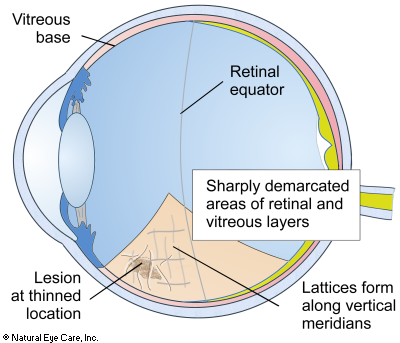
Lattice degeneration occurs between the retinal equator and the vitreous base.
The retinal equator is an imaginary boundary midway between the front and the back of the eyeball. The vitreous base lies toward the front of the eye where the retina, vitreous membrane, and pigmented layers firmly attach to each other. Lattice degeneration may show up as sharply demarcated areas of thinning. The thinning typically involves the vitreous and the inner layers of the retina. Sometimes thinning also occurs in the retinal pigment layer and rarely along the fine blood capillaries. The lattices usually form along the vertical meridians and perpendicular to the retinal equator.
Progression
Several things happen as the condition develops:
- the retina atrophies, forming a lesion, and becomes thinner due to obstructed blood supply
- larger blood vessels stiffen and become clogged
- the vitreous gel becomes more liquid over the retina lesion
- the vitreous contracts away from the retina and at the same time becomes more strongly attached to the retina, tearing it, detaching it, or causing holes and breaks in it
Sometimes retinal thinning is so great that holes develop through the retina at the lesion. The vitreous is then able to move through the retina into the space behind the retina contributing to retinal detachment. that a full-thickness hole atrophies through the retina at the lattice lesion. The overlying liquefied vitreous has the ability to pass through the hole into the subretinal space and for 2% of patients, leads to "rhegmatogenous" retinal detachment. In this case the fluid is accumulating between the retina and the pigment layer (RPE).
Symptoms
Patients are usually over 20 and rarely have symptoms, except for possibly noticing flashing lights (photopsia), a sudden onset of eye floaters, or partial loss of peripheral vision. Patients often have myopia (nearsightedness).
Causes
Heredity is likely a risk factor. A family history and certain variants in the COL4A4 gene may be risk factors. Lattice is inherited in an autosomal dominant manner; the affected parent having one mutated gene can pass it on to a child.
Myopia increases risk. Lattice is associated with those who have high myopic eyes, and its prevalence may be associated with increasing axial length, reaching 15% in the longest eyes. This is especially true of axial eye lengths between 29–30mm and 25–27mm.
Poor circulation. Lattice degeneration may also be linked to an insufficient blood supply or a blood supply with insufficient nutrients reaching the retina. From the front of the eye, to the retinal equator, the retina is supplied with nutrients by the posterior ciliary artery. When its circulation is degraded or obstructed, a "watershed zone" develops where there are fewer microcapillaries.
Other conditions. Researchers have also found a high rate of lattice degeneration in patients with full-thickness macular holes.
 See Vitamins & Supplements to support the retina and overall eye
health.
See Vitamins & Supplements to support the retina and overall eye
health.
Conventional Treatment
No standardized treatment exists for lattice degeneration. Clinical studies of interventions to prevent retinal detachment in lattice patients have been evaluated, but reviewers found that controlled trials were lacking, and no conclusions could be drawn. In certain cases where retinal holes or tears are present, a doctor might recommend laser photocoagulation or cryotherapy (extreme cold laser therapy), with the goal of sealing the area surrounding the tear. What mode is chosen depends on the location of the tear and whether there is fluid associated with it.
In most cases of lattice degeneration, no treatment is necessary. Treatment is recommended when a retinal tear occurs, if the other eye has had a retinal detachment, or if there is a strong family history of retinal detachments. Surgical intervention may be required if vitreous fluid is found to be leaking into the retina, which can complicate the lattice and atrophic holes, or if it is found in a patient who has suffered a previous retinal detachment (in an opposite eye).
Preventative or prophylactic treatment is indicated if there are tractional (pulling) tears due to vitreous detachment, or lesions are present in one eye when there is a retinal detachment in the other eye.
Self Help
Since poor circulation and nutrient deficiency have been identified as possible contributing causes for lattice degeneration, there may be natural ways to improve these situations, thereby boosting retinal health. Even in the case where lattice degeneration is inherited, the body is still trying to maintain healthy vision. So targeted supplements (antioxidants, in particular) and a healthy lifestyle can help to stop or slow down the progression of the disease and support healthy vision. Certain nutrients such as lutein, zeaxanthin,omega-3 fatty acids, vitamin D3, and herbs such as ginkgo or bilberry may be helpful.
Daily juicing of organic vegetables and fruits. Our recipe to support retinal health is a combination of the following: ginger, garlic, parsley, leeks, beets, cabbage, carrots, spinach, celery, apples, grapes, raspberries, lemon, chlorophyll, wheat grasses - (not too much fruit). See more on juicing.
Lattice Degeneration News
Want to learn more? See our blog news on lattice degeneration.
Related Conditions
- Lattice degeneration occurs more frequently (40% more) of patients with retinal detachment.
- Degenerative myopia, which is similar to macular degeneration
- Marfan's syndrome - this is a life-threatening disorder of connective tissue which can affect body systems, such as the heart. Damage due to Marfan can manifest as retinal detachment, dislocated lenses, nearsightedness, astigmatism, binocular conditions, glaucoma, and cataracts in children. 75% of cases are genetically caused.
- Stickler syndrome - another genetically-based disorder, is characterized by a somewhat flattened face. Stickler is a joint disorder that affects vision, hearing and joint problems. It is also known as progressive arthro-ophthalmopathy.
- Ehlers-Danlos syndrome - is another condition involving collagen that is too flexible resulting in loose joint dislocations, fragile skin, poor muscle tone. The eye (especially the cornea and sclera, is comprised of mostly connective tissue, and like lattice degeneration, this condition can result in retinal detachment.


{kind=link}